Aaron T. Beck’s cognitive model is a widely used model of depression explained using a cognitive framework. It explains how negative thoughts and a biased interpretation of events effect a person suffering from depression.
In this article, we introduce the key features of Beck’s cognitive model, followed by a summary of major developments in its evolution and finally discuss its strengths and limitations as a theory of depression.


Features of the cognitive model
Beck’s cognitive model (Beck, 1967) comprises a triad of automatic negative thoughts or schemas by the subject, that includes dysfunctional thoughts about themselves, the world and the future. These schemas are often formed by earlier experiences in one’s life, may be latent but get activated by adverse events in one’s environment.
For example, a subject may have failed or performed badly in an academic test, leading to negative thoughts such as
‘I do not deserve to pass this course’ (negative thought about themselves)
‘this course is too complicated to understand’ (negative thought about the world)
‘I shall never be able to pass this course’ (negative thought about the future).
The subjects may also have cognitive distortions or biases in their thinking that lead them to pay selective attention to the negative aspects of situations, while ignoring any positive aspects.
Some examples of such cognitive distortions include:
- overgeneralization (making a generalized conclusion or inference based on only a few events)
- selective abstraction (drawing conclusions about the situation on the basis of just a tiny bit of evidence)
- magnification (focusing on the negative aspects of the situation)
- minimization (downplaying the positive aspects of the situation)
- personalization (blaming oneself for causing the situation, to the exclusion of other factors).
These biases result in a pessimistic explanatory style, through which the depressed persons view and explain everything through a pessimistic lens. All of these factors together maintain the cycle of negative thoughts that may cause the subject to remain in a state of depression or drive episodes of depression.
Evolution of Beck’s cognitive model
Beck’s original cognitive model has evolved over time, with various additions to the model being made by Beck himself and by other psychologists (Beck, 2019).
Aaron Beck started his career as a psychoanalyst. In the early 1960s, he started to test the hypothesis, derived from psychoanalytical theory, that depression is the result of inward hostility and a need to suffer that would manifest in a depressed person’s dreams. However, he could not find enough evidence to support this hypothesis. From interviews with depressed patients, Beck realized they had one thing in common, which was automatic negative thoughts along with negative emotions. This led him to explore the relationship between negative thoughts and emotions, leading to the development of the cognitive model (Beck, 1967). In this, Beck was also inspired by Ellis’ Rational Emotive Behaviour Therapy (REBT) (Ellis, 1957).
Beck further incorporated the behavioral component from behaviorism (Watson, 1913) into the original cognitive model, showing how actions and behaviors were also influenced by negative thoughts. This led to the development of a therapy called Cognitive Behavioral Therapy or CBT (Rush et al., 1975, Beck, 2011) that incorporated behavioral elements.
Beck then collaborated with various psychologists such as A. John Rush at the University of Pennsylvania and attempted to put the cognitive model on a solid evidence-based footing, developing tools such as the Beck Depression Inventory (Beck, 1984) and Dysfunctional Attitude Scale (Beck et al., 1991) to measure the degree of depression and negative attitudes in patients and showing that the therapy based on the cognitive model was as good as antidepressant drugs in randomized controlled trials (Beck et al., 1979).
Later, physiological elements were added to the original cognitive model, showing how negative thoughts can also affect the physiology of the body (Beck, 2008), give rise to changes in the brain and effect the release of stress related hormones such as cortisol and serotonin. The cognitive model was also applied to other conditions such as anxiety disorders (Wells, 1999), phobias (Beck et al., 2005) and bipolar disorders (Mansell et al., 2007).
Beck and Haigh (2014) developed the generic cognitive model to generalize and advance its findings and approaches across a wide range of disorders and environmental triggers, adding an expanded theory of modes and early schema activation.
Recently, Beck and colleagues developed the unified model of depression (Beck & Bredemeier, 2016) that added perspectives for depression from various fields including genetics and evolutionary biology.
Rief and Joormann (2019) have recently analyzed what is meant by the “cognition” aspect of the cognitive model of depression and hypothesized that it refers more to dysfunctional expectations rather than just negative thoughts.
How can Cognitive Behavior Therapy (CBT) be applied to Depression
Cognitive Behavior Therapy (CBT) is a therapy based on the cognitive model. It suggests different practices in which we can identify negative thoughts and behaviors, challenge the hidden assumptions and beliefs that cause them and formulate action plans to help with them. It can be applied for depression as well as anxiety and many other disorders.
In this article, we only provide a high level overview of how CBT might be applied. It is always advised to consult a qualified CBT therapist whenever one feels they might like to try out CBT as a treatment for depression.
Some of the ways in which CBT can be applied to help people with depression are the following:
Identifying negative thoughts, emotions and behaviors: The client is encouraged to monitor their automatic thoughts, emotions and behaviors that occur every day.
This can be done by the clients reflecting and writing down their thoughts in different situations or at different times of the day, especially when they are feeling depressed. The help of structured questionnaires, worksheets and forms can be taken for the same. The client is enabled to make a connection between the negative thoughts and depression.
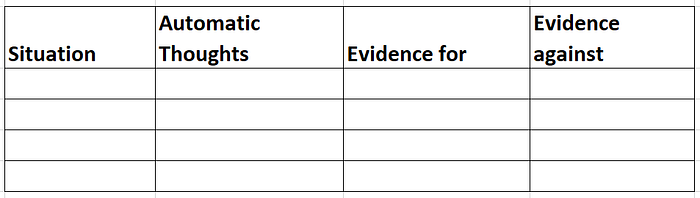
Challenging negative thought patterns: Once the negative thoughts are identified, the client is encouraged to examine each thought and challenge the assumptions underlying such thoughts and emotions, sometimes with evidence of the opposite.
For example, if the thought is “I am a failure”, the client is encouraged to bring to mind instances in their life where they have been successful and not a failure. For example, they might be handling their finances quite well or taking care of their family. This can also be done for events that occurred in the client’s life during the day or the week. The client is enabled to reframe the automatic negative thoughts into more realistic appraisals about the situation or event.
Action plans and activities to strengthen positive behaviors: The client is encouraged to cultivate positive emotions and experiences. This can be done by encouraging them to bring to mind positive memories and positive incidents during the day. This enables them to focus more on the positive incidents rather than only the negative ones.
Action plans can be formulated, consisting of small activities throughout the day that cause the clients to have a sense of accomplishment and achievement, thus encouraging positive thoughts.
Inculcating skills for problem solving and stress management: The CBT therapist encourages the client to inculcate skills to deal with problems and stress in a better way.
Some practices for stress management can include deep breathing and mindfulness meditation.


Strengths of the cognitive model as a theory of depression
One study by Strunk and Adler (2009) tested the assumption of the cognitive model that depressed patients had cognitive biases. They found that in a few tasks, people with depression showed evidence of substantial pessimistic bias, thus confirming the prediction of the cognitive model.
Another experiment by Alloy et al. (1999) tested the hypothesis that negative thinking styles led to more susceptibility to depression among college freshmen and found that they indeed made the subjects more vulnerable to depression. Another study by Haeffel (2008) found that negative thinking styles among college freshmen made their roommates more vulnerable to depression as well, showing that depression could be induced by talking to people with negative thoughts. A further study by Bates et al. (1999) found that simply reading negative mood statements could induce depressive states in otherwise normal subjects, further validating the cognitive model.
A study among recent Korean migrants in Australia (Oei & Kwon, 2007) found that a cognitive model was more successful at explaining and predicting depression and anxiety after negative life events than competing models including the symptom model and linear mediation model. Another study (Esbensen & Benson, 2007) evaluated the cognitive triad among adults with intellectual disability, and found that a depressed mood did predict a negative cognitive triad but not vice versa.
A study by Disner et al. (2011) found support for neural mechanisms for depression, including biased views and negative schemas, as explained by the cognitive model. For example, the brain regions and pathways responsible for emotion and cognition, such as the amygdala and cortex, were found to be activated in maintaining negative thoughts in depressed patients.
The cognitive model has been applied practically as a treatment for depression. Therapies based on the cognitive model including CBT (Elkin et al.,1989, Cuijpers et al., 2013) and its variants such as rumination focused CBT (Watkins et al., 2007) and mindfulness-based CBT (Kishita et al., 2017) have shown evidence of their effectiveness in treating depression in meta-analysis. Similarly, a study by Butler and Beck (2000) showed that 80% patients in a randomized control trial benefited from a cognitive approach to treating depression.
Limitations of the cognitive model of depression
There are a number of limitations of the cognitive model as a theory of depression. Although the cognitive model does seem to explain depression, exactly why the model works is still not clear considering the scientific evidence. Some questions still remain unanswered, such as, does negative thinking cause or maintain depression, or is it simply a phenomenon correlated with, or a by-product of depression?
Also, the cognitive model does not explain adequately all the phenomena associated with depression, such as rumination in patients with long-term depression. It does not explain hallucinations and certain types of delusions in depressed patients such as Cotard’s delusion, which makes people feel they do not exist (Mendhekar & Gupta, 2005). It does not account for differences in how depression varies based on gender differences (Hyde et al., 2008, Ryba & Hopko, 2012) and age differences (Kessler et al., 2010) and differences in existing co-morbidities in patients (Kang et al., 2015). Furthermore, there are a number of findings that show that other mechanisms than those explained by the cognitive model may be related to depression, including molecular and cellular mechanisms (Fox & Lobo, 2019), neurocognitive mechanisms (Clark et al., 2009, Hodes et al., 2015) and hormone imbalance in the brain (Tafet et al., 2001). Overall, the cognitive model does not explain how genetic, biological and environmental factors can make some people more vulnerable to depression than others.
The cognitive model also does not explain how antidepressant drugs (Bartoli et al., 2021) have sometimes proven as effective as the best therapies based on the cognitive model. If negative thinking styles are mainly the cause of depression, then how can medication be effective in treating it? Even placebos have been proven effective in managing depression in some studies (Kirsch, 2019, Cuijpers & Cristea, 2015).
Genetically modified mice (Castagne et al., 2011) and other animals have been long used in laboratories to study depression linked behavior and explore treatments for depressions. The cognitive model does not account for how such animals can display depression like behavior (Wang et al., 2017), considering they are not known to have the same cognitive abilities as humans.
Conclusion
Opinion is divided as to whether the cognitive model is the best way to explain depression. It certainly has evidence in its favor such as neural correlates and good performance in managing depression among patients using therapies based on the model.
On the other hand, phenomena such as differences in depression among people are not explained by the cognitive model. Why the model works as well as it does is still not quite clear. Despite this, as a benchmark model that is well proven by evidence of its effectiveness, the cognitive model is probably the best we have.
References
Alloy, L. B., Abramson, L. Y., & Francis, E. L. (1999). Do negative cognitive styles confer vulnerability to depression? Current Directions in Psychological Science, 8(4), 128–132. https://doi.org/10.1111/1467-8721.00030
Bartoli, F., Cavaleri, D., Bachi, B., Moretti, F., Riboldi, I., Crocamo, C., & Carrà, G. (2021). Repurposed drugs as adjunctive treatments for mania and bipolar depression: A meta-review and critical appraisal of meta-analyses of randomized placebo-controlled trials. Journal of psychiatric research, 143, 230–238. https://doi.org/10.1016/j.jpsychires.2021.09.018
Bates, G. W., Thompson, J. C., & Flanagan, C. (1999). The effectiveness of individual versus group induction of depressed mood. The Journal of Psychology, 133(3), 245–252. https://doi.org/10.1080/00223989909599737
Beck, A. T. (1967). Depression: Causes and treatment. Philadelphia: University of Pennsylvania Press.
Beck, A. T., Rush A. J., Shaw B. F. & Emery G. (1979) Cognitive Therapy of Depression, Guildford Press.
Beck, A. T., Emery, G., & Greenberg, R. L. (2005). Anxiety disorders and phobias: A cognitive perspective. Basic Books.
Beck, A. T. (2019). A 60-year evolution of cognitive theory and therapy. Perspectives on Psychological Science, 14(1), 16–20. https://journals.sagepub.com/doi/10.1177/1745691618804187
Beck, A. T., & Steer, R. A. (1984). Internal consistencies of the original and revised Beck Depression Inventory. Journal of clinical psychology, 40(6), 1365–1367. https://doi.org/10.1016/j.jpsychires.2021.09.018
Beck, A. T., & Bredemeier, K. (2016). A unified model of depression: Integrating clinical, cognitive, biological, and evolutionary perspectives. Clinical Psychological Science, 4(4), 596–619. https://doi.org/10.1177/2167702616628523
Beck A. T. (2008). The evolution of the cognitive model of depression and its neurobiological correlates. The American journal of psychiatry, 165(8), 969–977. https://doi.org/10.1176/appi.ajp.2008.08050721
Beck, A. T., & Haigh, E. A. (2014). Advances in cognitive theory and therapy: the generic cognitive model. Annual review of clinical psychology, 10, 1–24. https://doi.org/10.1146/annurev-clinpsy-032813-153734
Beck, J. S. (2011). Cognitive behavior therapy: Basics and beyond (2nd ed.). Guilford Press.
Butler, A. C., & Beck, J. S. (2000). Cognitive therapy outcomes: A review of meta-analyses. Journal of the Norwegian Psychological Association, 37, 1–9.
Castagné, V., Moser, P., Roux, S., & Porsolt, R. D. (2011). Rodent models of depression: forced swim and tail suspension behavioral despair tests in rats and mice. Current protocols in neuroscience, Chapter 8. https://doi.org/10.1002/0471142301.ns0810as55
Clark, L., Chamberlain, S. R., & Sahakian, B. J. (2009). Neurocognitive mechanisms in depression: implications for treatment. Annual review of neuroscience, 32, 57–74. https://doi.org/10.1146/annurev.neuro.31.060407.125618
Cuijpers, P., & Cristea, I. A. (2015). What if a placebo effect explained all the activity of depression treatments?. World psychiatry : official journal of the World Psychiatric Association (WPA), 14(3), 310–311. https://doi.org/10.1002/wps.20249
Cuijpers, P., Berking, M., Andersson, G., Quigley , L., Kleiboer, A., & Dobson, K. S. (2013). A meta-analysis of cognitive-behavioural therapy for adult depression, alone and in comparison with other treatments. The Canadian Journal of Psychiatry, 58(7), 376–385. https://journals.sagepub.com/doi/10.1177/070674371305800702
Disner, S. G., Beevers, C. G., Haigh, E. A., & Beck, A. T. (2011). Neural mechanisms of the cognitive model of depression. Nature reviews. Neuroscience, 12(8), 467–477. https://doi.org/10.1038/nrn3027
Ellis, A. (1957). Rational Psychotherapy and Individual Psychology. Journal of Individual Psychology, 13: 38–44. https://doi.org/10.1080/00221309.1958.9710170
Elkin, I., Shea, M. T., Watkins, J. T., Imber, S. D., Sotsky, S. M., Collins, J. F., … & Parloff, M. B. (1989). National Institute of Mental Health treatment of depression collaborative research program: General effectiveness of treatments. Archives of general psychiatry, 46(11), 971–982. https://doi.org/10.1001/archpsyc.1989.01810110013002
Esbensen, A. J., & Benson, B. A. (2007). An evaluation of Beck’s cognitive theory of depression in adults with intellectual disability. Journal of Intellectual Disability Research, 51(1), 14–24. https://onlinelibrary.wiley.com/doi/10.1111/j.1365-2788.2006.00860.x
Fox, M. E., & Lobo, M. K. (2019). The molecular and cellular mechanisms of depression: a focus on reward circuitry. Molecular psychiatry, 24(12), 1798–1815. https://doi.org/10.1038/s41380-019-0415-3
Haeffel, G. J., Gibb, B. E., Metalsky, G. I., Alloy, L. B., Abramson, L. Y., Hankin, B. L., Joiner T. E. Jr., & Swendsen, J. D. (2008). Measuring cognitive vulnerability to depression: Development and validation of the cognitive style questionnaire. Clinical psychology review, 28(5), 824–836. https://doi.org/10.1016/j.cpr.2007.12.001
Hodes, G. E., Kana, V., Menard, C., Merad, M., & Russo, S. J. (2015). Neuroimmune mechanisms of depression. Nature neuroscience, 18(10), 1386–1393. https://doi.org/10.1038/nn.4113
Hyde, J. S., Mezulis, A. H., & Abramson, L. Y. (2008). The ABCs of depression: integrating affective, biological, and cognitive models to explain the emergence of the gender difference in depression. Psychological review, 115(2), 291–313. https://doi.org/10.1037/0033-295X.115.2.291
Kang, H. J., Kim, S. Y., Bae, K. Y., Kim, S. W., Shin, I. S., Yoon, J. S., & Kim, J. M. (2015). Comorbidity of depression with physical disorders: research and clinical implications. Chonnam medical journal, 51(1), 8–18. https://doi.org/10.4068/cmj.2015.51.1.8
Kessler, R. C., Birnbaum, H., Bromet, E., Hwang, I., Sampson, N., & Shahly, V. (2010). Age differences in major depression: results from the National Comorbidity Survey Replication (NCS-R). Psychological medicine, 40(2), 225–237. https://doi.org/10.1017/S0033291709990213
Kirsch I. (2019). Placebo Effect in the Treatment of Depression and Anxiety. Frontiers in psychiatry, 10, 407. https://doi.org/10.3389/fpsyt.2019.00407
Kishita, N., Takei, Y., & Stewart, I. (2017). A meta‐analysis of third wave mindfulness‐based cognitive behavioral therapies for older people. International journal of geriatric psychiatry, 32(12), 1352–1361. https://onlinelibrary.wiley.com/doi/10.1002/gps.4621
Mansell, W., Morrison, A. P., Reid, G., Lowens, I., & Tai, S. (2007). The interpretation of, and responses to, changes in internal states: An integrative cognitive model of mood swings and bipolar disorders. Behavioural and Cognitive Psychotherapy, 35(5), 515–539.
Mendhekar, D. N., & Gupta, N. (2005). Recurrent postictal depression with Cotard delusion. The Indian Journal of Pediatrics, 72(6), 529–531. https://link.springer.com/article/10.1007%2FBF02724434
Oei, T. P., & Kwon, S. M. (2007). Evaluation of the integrated cognitive model of depression and its specificity in a migrant population. Depression and anxiety, 24(2), 112–123. https://doi.org/10.1002/da.20225
Rief, W., & Joormann, J. (2019). Revisiting the cognitive model of depression: The role of expectations. Clinical Psychology in Europe, 1(1), 1–19. https://cpe.psychopen.eu/index.php/cpe/article/view/2373
Rush, A. J., Khatami, M., & Beck, A. T. (1975). Cognitive and behavior therapy in chronic depression. Behavior Therapy, 6(3), 398–404. https://doi.org/10.1016/S0005-7894(75)80116-X
Ryba, M. M., & Hopko, D. R. (2012). Gender Differences in Depression: Assessing Mediational Effects of Overt Behaviors and Environmental Reward through Daily Diary Monitoring. Depression research and treatment, 2012, 865679. https://doi.org/10.1155/2012/865679
Strunk, D. R., & Adler, A. D. (2009). Cognitive biases in three prediction tasks: a test of the cognitive model of depression. Behaviour research and therapy, 47(1), 34–40. https://doi.org/10.1016/j.brat.2008.10.008
Tafet, G. E., Idoyaga-Vargas, V. P., Abulafia, D. P., Calandria, J. M., Roffman, S. S., Chiovetta, A., & Shinitzky, M. (2001). Correlation between cortisol level and serotonin uptake in patients with chronic stress and depression. Cognitive, affective & behavioral neuroscience, 1(4), 388–393. https://doi.org/10.3758/cabn.1.4.388
Wang, Q., Timberlake, M. A., 2nd, Prall, K., & Dwivedi, Y. (2017). The recent progress in animal models of depression. Progress in neuro-psychopharmacology & biological psychiatry, 77, 99–109. https://doi.org/10.1016/j.pnpbp.2017.04.008
Watkins, E., Scott, J., Wingrove, J., Rimes, K., Bathurst, N., Steiner, H., Kennell-Webb, S., Moulds, M., & Malliaris, Y. (2007). Rumination-focused cognitive behaviour therapy for residual depression: a case series. Behaviour research and therapy, 45(9), 2144–2154. https://doi.org/10.1016/j.brat.2006.09.018
Watson, J. B. (1913). Psychology as the behaviorist views it. Psychological Review, 20(2), 158–177. https://doi.org/10.1037/h0074428
Wells A. (1999). A cognitive model of generalized anxiety disorder. Behavior modification, 23(4), 526–555. https://doi.org/10.1177/0145445599234002
